| « COVID: If there is no virus, why are people dying? | The coronavirus: using "animal models" as proof of infection; another lie » |
Debunking the 95% Vaccine Effectiveness Rate Propaganda of the Two Experimental, Untested for Long-term Safety, mRNA-containing Covid-19 Vaccines

By Gary G. Kohls, MD
The Effectiveness of Pfizer’s and Moderna’s Covid-19 Vaccines Have Been Grossly Over-rated by Big Pharma, Big Government and Big Media
Compelling Reasons to Delay Being Inoculated with What May Turn Out to be Useless – or Worse - Vaccines
(Also Pointing Out Minnesota’s 99.6% Survival Rates Among Non-Long-term Care Facility Patients)
Question: What would any aware person think if the headlines – and the claims from the talking heads - about the two Covid-19 vaccine clinical trials had read:
“Shot Reduces COVID-19 Risk by Less Than 1%” rather than “COVID-19 Shot 95% Effective”?
The answer to the question is obvious: There would be no long lines at the vaccination centers and the level of vaccine hesitancy would rise above the current 50+% that already exists among the informed, thoughtful, propaganda-resistant population.
Read on to see some of the reasons why people need not freak out if they can’t get one of Big Pharma’s experimental vaccines (which are still not proven to be safe - OR even effective –long-term.
______
In November 2020, Peter Doshi, MD, an associate editor with the British Medical Journal (The BMJ) wrote an important article that was published in his journal that debunked the propagandistic claim from Pfizer and Moderna (and widely propagated by the HHS, the NIH, the CDC, the NIAID, the FDA and even Anthony Fauci) that their fast-tracked, experimental vaccines were “95% effective”.
The truth of the matter, of course, is that the actual/absolute vaccine efficacy rates are actually less than 1%! The full article explaining the ruse is available at the following site:
In my opinion, some of the most pertinent information comes in the online comments that follow articles, especially in scientific articles. Below is such a sampling of comments to the Doshi article.
Please pay close attention to the graphs, which seem to be NEVER displayed, spoken of or published in mainstream media outlets; nor are the unwelcome truths illustrated in the graphs ever pointed out in the propagandistic advertisements that come far too often from public health departments and the CDC.
______
“So, the biggest misgiving in the trial is that the "95% effective" stat is taken from the natural infection rate (0.5 - 1% say) which is only 200 people or so possible in each arm. The vaccine makes you feel like you have flu for a while, maybe worse - so you lay low for a good time and don't do things you'd normally do. So that changes your exposure, and the infection rate is lower. You also take meds (such as fever meds that are also pain-relieving) to get over the symptoms of the vaccine - same as you do for a cold (clinical trial members were even told to take such drugs in the trial leaflet) but medications would ameliorate some Covid-19 symptoms (like fever, chills, fatigue, headache and muscle aching) - thus skewing the results in favor of the vaccine trialists, given the fact that the placebo trialists wouldn’t be taking such medications.”
______
“The author reports an Absolute Risk Reduction for the vaccines (treatment versus placebo) of less than 1%. The Number Needed to Vaccinate (NNV) is, by definition, the inverse of the Absolute Risk Reduction (ARR).
“So, the NNV is greater than 100. (The inverse of 1/100 = 100). That is, more than 100 people would have to take the vaccine before one extra person would be benefited from getting the two inoculations.
“This is a very poor Number Needed to Treat (NNT).
“The Oxford/Astra/Zeneca trial was so rushed that it couldn't even get the dosages right. A bad vaccine – combined with a bad PCR test for diagnosing Covid-19 - is worse than no vaccine at all.”
______
“Understanding the difference between the Relative vs Absolute risk of a drug or vaccine is a really important point that needs to be made.
“The Relative Risk Reduction (RRR) statistic is commonly used as a propaganda/advertising tool by pharmaceutical companies to make a useless drug or vaccine appear far more effective than it actually is. The deceptive RRR statistic intentionally over-states the results of the clinical study that make bad drugs and vaccines easier to market.
“The far more logical - and accurate - Absolute Risk Reduction (AAR) statistic is essentially never used by the pharmaceutical industry because it is too honest and will result in more difficulty in selling the product to the public.
“There were 44,000 people in the two arms of the Pfizer vaccine trial. Here are the raw statistics of the placebo group as compared to the vaccine group: (It should be noted that the primary endpoints in both studies were cough, fever, headache, muscle pain and chills [plus PCR testing, which commonly causes false positives.)
“The Pfizer placebo group: 162/22,000 = 0.736% were diagnosed with Covid.
“The Pfizer vaccine group: 8/22,000 = 0.036% were diagnosed with Covid.
“In calculating the ARR, one subtracts 0.036% from 0.736% which represents a difference of only 0.7%, which if far below the heavily advertised, deceptive RRR of 95%.”
______
One commenter accurately stated: “I am not a statistician, but I don't understand how this (ie, the 95% effectiveness rate) could ever be statistically significant. Even the slightest change in mean age between the groups would totally invalidate the study.”
______
Understanding the difference between Relative Risk Reduction and Absolute Risk Reduction (95% vs o.7%)
By Claus Rinner – December 13, 2020
from: https://gis.blog.ryerson.ca...

Calculation of Relative Risk Reduction and Absolute Risk Reduction for COVID-19 vaccine trials.
“The concept of risk, and our ability to assess risk, has also made the headlines in the context of the COVID-19 vaccine trials. Using data from a Nov 26 opinion piece in the British Medical Journal (BMJ), we can see that vaccine efficacy in terms of the “relative” reduction of the risk of getting ill is around 95%.
“For example, in the Pfizer trial, assuming an equal split of the 44,000 participants into the vaccine and placebo groups, 0.74% of the placebo group fell ill but only 0.04% of the vaccinated participants did. The relative risk reduction is calculated as the difference between these two incidences (0.7%) divided by the placebo value (0.74%), arriving at the conclusion that 95% of COVID-19 could be avoided if people got immunized.
“However, there is another way of looking that the same data: The risk reduction in absolute terms is only 0.7%, from an already very low risk of 0.74% to a minimal risk of 0.04%.
“In terms of publicly presenting and discussing the vaccine trial results, a 2019 article in the Drug and Therapeutics Bulletin is revealing. Box 3 explains the difference between absolute and relative risk reduction. Note the author’s statement ‘Relative risks, then, can exaggerate the perception of difference, and this is especially prominent when the absolute risks are very small.’
“What would you think if the headlines about the two Covid-19 vaccine clinical trials had read: ‘Shot Reduces COVID-19 Risk by 0.7%’ instead of ‘COVID-19 Shot 95% Effective’?”
“The author of ‘How to Communicate Evidence to Patients’, Dr. Alexandra Freeman, advocates for reporting multiple metrics for better context. With respect to the ongoing pandemic, the powers-that-be should ensure transparent communication of scientific evidence. This also includes a host of other issues with the vaccine trials that Dr. Peter Doshi raises in the above-cited BMJ commentary.”
______
Covid-19 has a survival rate of over 99.6% in non-long-term care (LTC) patients. Why the rush to a vaccine?
From: coleenrowley
The survival rate is >99% for those less than 65 years old. Here is the CDC and the Minnesota Department of Health's 2020 data, as of December 2, 2020:
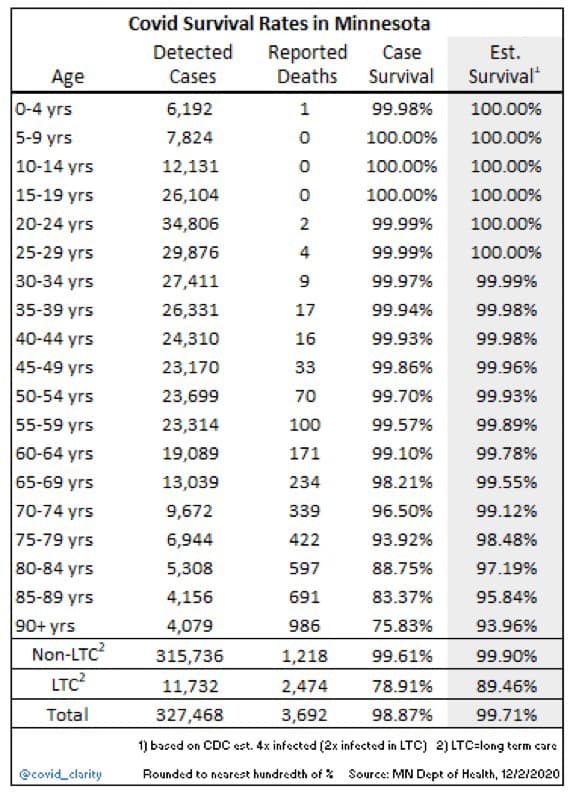
“Survival rates are over 99% actually. And an infection rate at any given time, not taking into account the false positive cases, is a tiny fraction of 1% of the population. In fact, it took one year for this modern "black death" to reach 1% of the population. (What kind of an epidemic is that?)”
-###-
Dr Gary G. Kohls lives in the USA and writes a weekly column, entitled Duty to Warn, for the Duluth Reader, Duluth, Minnesota’s alternative newsweekly magazine. His columns deal with the dangers of American Friendly Fascism, corporatism, Oligarchy, militarism, racism, malnutrition, and Big Pharma’s over-drugging and over-vaccinating agendas as well as other movements that threaten the environment, democracy, civility, health and the sustainability and livability of the planet and the future of the children. Dr. Kohls is a past member of Mind Freedom International, the International Center for the Study of Psychiatry and Psychology and the International Society for Traumatic Stress Studies and is a signatory to and/or an advocate of the principles of the Great Barrington Declaration, the World Doctors Alliance and Americas Front Line Doctors. His practice of holistic medicine mainly involved helping the survivors of psychiatry that had often been mis-diagnosed, over-diagnosed and always over-medicated with un-approved and un-tested-for-safety cocktails of neurotoxic psychiatric drugs that not only had sickened them but to which they had also become addicted. His Duty to Warn columns have been re-published around the world for the last decade. They deal frequently also deal with Big Vaccine’s over-vaccinating, Big Medicine’s over-screening, over-diagnosing and over-treating agendas Many of Dr Kohls’ columns have been archived at a number of websites, including:
http://duluthreader.com/search?search_term=Duty+to+Warn&p=2;
http://www.globalresearch.ca/author/gary-g-kohls
http://freepress.org/geographic-scope/national
https://www.lewrockwell.com/author/gary-g-kohls/?ptype=article; and
https://www.transcend.org/tms/author/?a=Gary%20G.%20Kohls,%20MD
No feedback yet
